
By Lam Nguyen, MD, Orthopedic Surgeon
 The spine is made up of bony blocks called the vertebrae. Between each vertebra are the intervertebral discs, which are composed of spongy materials that behave as shock absorbers in the spine. In addition to the intervertebral discs, the vertebrae are connected to each other via facet joints. The spinal canal runs through the vertebrae and contains the spinal cord and spinal nerves supplying sensation and strength to the legs.
The spine is made up of bony blocks called the vertebrae. Between each vertebra are the intervertebral discs, which are composed of spongy materials that behave as shock absorbers in the spine. In addition to the intervertebral discs, the vertebrae are connected to each other via facet joints. The spinal canal runs through the vertebrae and contains the spinal cord and spinal nerves supplying sensation and strength to the legs.
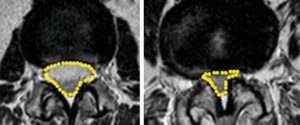
With aging, the intervertebral discs become less spongy and fluid-filled and their height collapses. As a result, the hardened discs bulge out into the spinal canal. When this occurs, the facet joints and ligaments are subjected to increased mechanical stresses. Overtime, the facet joints become arthritic (wear out, become inflamed, and form bony spurs) and the ligaments become thickened. The combination of the bulging discs, the formation of bony spurs, and the thickened ligaments all cause crowding or narrowing of the spinal canal, leading to pinching of the spinal nerve roots, a condition known as spinal stenosis.
Spinal stenosis affects many patients and is one of the most common reasons for spinal surgery in the aging population. Spinal stenosis does not necessarily cause symptoms. Many people can have significant stenosis on imaging studies but fail to have symptoms. This known fact highlights the importance of correlating the patient’s symptoms with radiographic findings.
The clinical presentation of lumbar spinal stenosis typically consists of back and leg pain. The leg pain may present in a specific distribution (such as sciatica where the pain runs down the back of the buttock, thigh, and leg), or it may presents as a generalized numbness, heaviness, cramping, burning, or weakness in the lower extremities. Rarely, bowel and/or bladder problems can occur if the narrowing is severe. Symptoms are often worse with prolonged standing or walking. Symptoms may come and go, and may vary in severity when present. Bending forward, sitting, or leaning forward while walking (such as leaning against a shopping cart) increases the space in the spinal canal and may lead to pain improvement and better walking tolerance.
The evaluation of lumbar spinal stenosis includes a thorough history and physical examination. Your physician will order imaging studies, including xrays and MRI and/or CT scan with or without contrast (known as CT myelogram) to confirm the presence, location, and severity of the spinal canal narrowing and nerve pinching. As mentioned earlier, because many patients have spinal stenosis (narrowing of the spinal canal and pinching of the spinal nerves) but are completely asymptomatic, it is crucial that your physician takes the time to make sure that your pain is not caused by another problem. It is unfortunate, but I have heard of numerous stories of patients who underwent spinal surgery without any pain relief only later to find out that their pain has been caused by arthritis in the hip or clogging of the large arteries in their abdomen and pelvis. When these patients later undergo a hip replacement surgery or stenting of their arteries, their leg pain then resolves. Make sure your physician takes the time to correlate your symptoms with your imaging findings, especially when your symptoms are not classic/characteristic for spinal lumbar stenosis.
Once it has been determined that lumbar spinal stenosis is the cause of your pain, the first line of treatment is nonsurgical. Nonsurgical treatments do not correct the spinal canal narrowing of spinal stenosis itself but may provide long-lasting pain control and improved life function without requiring more invasive treatment. A comprehensive program may require three or more months of supervised treatment.
Typically, nonsurgical treatment consists of Tylenol and/or nonsteroidal anti-inflammatory medications (such as ibuprofen or naproxen or prescription strength anti-inflammatory drugs). The nonsteroidal anti-
inflammatory drugs (NSAID’s) work well in that they reduce swelling and inflammation of the nerve roots. If your doctor prescribes NSAIDs, be on the look out for side effects such as gastrointestinal upsets or bleeding. Other medications with anti-inflammatory effects are also available. Steroid medications can be prescribed orally or by injections (such as an epidural injection of cortisone) for more severe back and leg pain because of their very powerful anti-inflammatory effect. Corticosteroids, like NSAIDs, can have side effects. Risks and benefits of this medication should be discussed with your physician.
A short course of narcotic medications is reserved for pain not controlled with other analgesics or NSAIDs. Only take the amount prescribed by your doctor. Side effects include nausea, constipation, dizziness and drowsiness, and use can result in addiction.
Medications like gabapentin (Neurontin) or pregabalin (Lyrica) may be prescribed by your physician for leg symptoms – particularly numbness, tingling, and burning. These medications have been shown to decrease nerve pain and improve walking tolerance for some patients.
Pain caused by spinal stenosis frequently results in activity avoidance. This results in reduced flexibility, strength and activity endurance. Therefore, your doctor may prescribe a course of physical therapy or exercise program. Everyday activities can become less challenging if flexibility, strength, and endurance are optimized.
When non-surgical treatments can no longer provide adequate and/or long-lasting relief from pain and improve function and quality of life, the patient may consider operative treatment. Surgery is also advised for patients who develop progressive leg weakness, or bowel and bladder problems.
Since spinal stenosis is a narrowing of the bony canal, the goal of the surgery is to open up the bony canal to improve available space for the nerves. This is called lumbar decompression surgery, or laminectomy. Surgery, when necessary, will reliably relieve the leg pain. The relief of back pain is less predictable since the surgery does not cure the underlying arthritis condition in the spine. Patients are allowed to return to most activities within about 6 weeks. Postoperative rehabilitation may be advised to assist in return to normal activities.
Sometimes, in spinal stenosis, the vertebrae shift or slip in relation to each other (spondylolisthesis). Abnormal motion (instability) may then occur between the vertebrae, further contributing to the narrowing of the canal and pinching of the spinal nerves. In such cases, spinal fusion surgery may be required in addition to decompression in order to stabilize the involved vertebrae. A fusion is performed by placing bone graft, bone substitute, and/or instrumentation (rods and screws) between the vertebrae being fused. Fusion can be performed from the front (anterior approach) or from the back (posterior approach), or may require both anterior and posterior approaches. The choice of approach is influenced by many technical factors. Your doctor will decide the best surgery for you, depending on the need for bony spur removal, anatomic variations, and the degree of instability.
KWOC
For more information on their services and organization,
please visit their website at www.Kwoc.net.
941-893-6447